Bowel Polyps
What is a bowel polyp?
A bowel polyp is an abnormal growth of tissue growing on the wall of the bowel (colon). If polyps are left for years, a small number may develop into bowel cancer. Bowel polyps can be detected at the time of colonoscopy and can usually be removed completely and safely, eliminating the chance for that polyp to develop into a cancer.
About half of all adult Australians develop a bowel polyp during their lifetime. Although polyps are very common, they rarely produce symptoms and are usually discovered by chance at the time of colonoscopy or after a positive faecal occult blood test (FOBT).
Most people develop just a few polyps but a small number of people, who have a ‘polyposis syndrome’, may develop 50 polyps or more and will need frequent colonoscopies to remove all these polyps.
What does a bowel polyp look like?
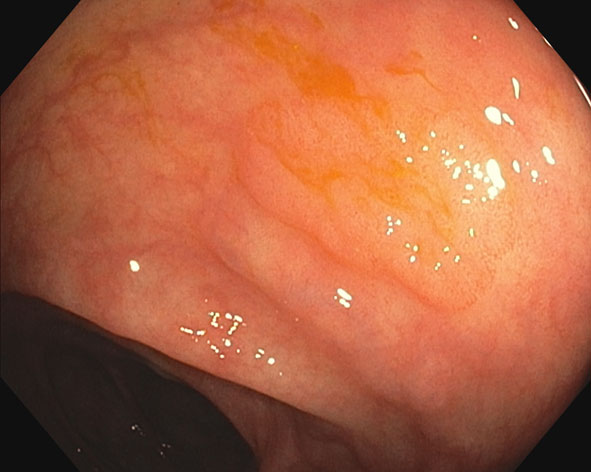
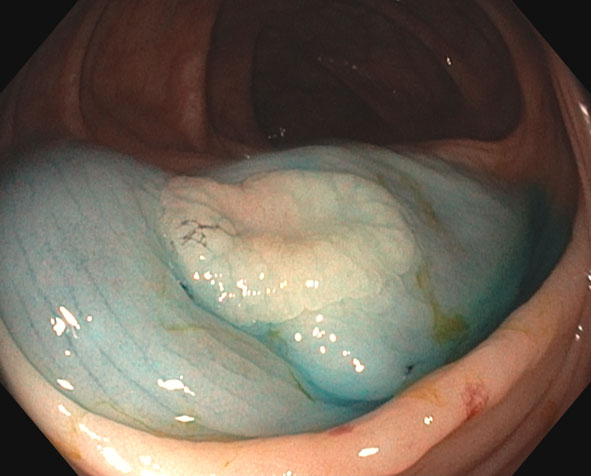
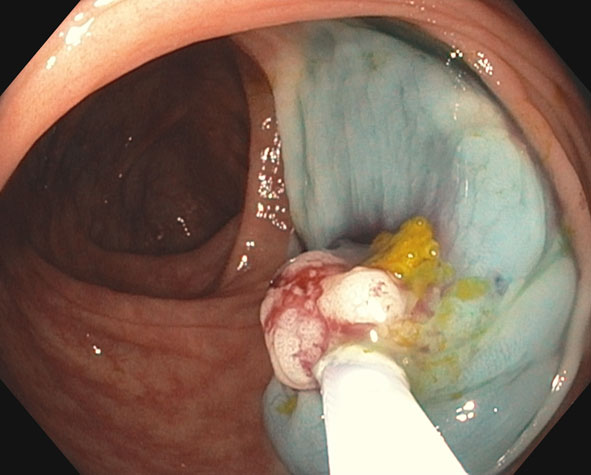
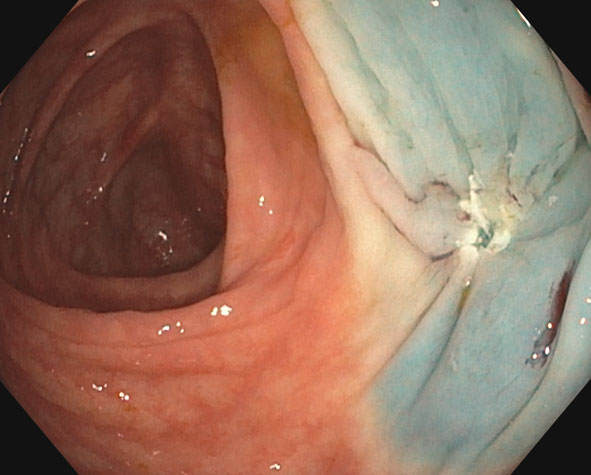
Some polyps are a fleshy nodule on a stalk – these are called pedunculated polyps. Some polyps are flat lesions, barely raised above the surrounding bowel lining – these are called sessile polyps.
Many polyps are quite small, only a few mm in size. Most are less than 1cm however they may be more than 5cm in size. The size does not necessarily correlate with the risk of a polyp having already developed into cancer, although it is rare for a polyp less than 1cm to contain cancer.
What are the different sorts of bowel polyps?
There are a number of different types of polyps in the colon.
- Tubular adenomas are the most common type of polyp and they have the potential to develop into bowel cancer, although most will not. If found, they need to be removed.
- Sessile serrated adenomas are typically very flat polyps that are more common on the right side of the bowel. They can be very difficult to detect and some may develop into cancer. If found, they need to be removed.
- Hyperplastic polyps are usually small and typically in the left colon, the sigmoid colon and rectum. They do not carry a risk of developing into cancer, except in patients with a rare syndrome of multiple hyperplastic polyps. It is not always possible to distinguish a hyperplastic polyp from other polyps, so they are often removed to allow microscopic evaluation.
- Inflammatory polyps generally occur in patients who have had inflammation of the bowel such as ulcerative colitis or Crohn’s disease. They do not carry a risk of developing into cancer.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}